

Helping you to manage your health
For information on how best to be seen at the Surgery, select the service or condition you require.
Who to see: GP, Physician Associate or Advanced Nurse Practitioner
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: GP, Physician Associate or Asthma Nurse
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: GP, Physician Associate/Advanced Nurse Practitioner or Mental Health Nurse
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: GP, Physician Associate/Advanced Nurse Practitioner or In-House Physiotherapist
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: Health Care Assistant
Advice: Nurse/Health Care Assistant will consult the GP as necessary.
Advice: You can take your BP in either Surgery with the machine in the waiting room, please hand results to Receptionist
Who to see: Phlebotomist
Advice: Clinics are held daily at various times. Appointments for blood test must have been requested by your doctor or other health care professional.
For warfarin monitoring it is preferred for all samples to be taken at the beginning of the week. If you are in doubt please call to speak to one of our nurses who will advise you.
Who to see: Bath & North East Somerset Council
Advice: Please call 01225 477133 or email blue_badge@bathnes.gov.uk. Blue Badge application form can be found here: www.bathnes.gov.uk
Who to see: Community Pharmacy Referral
Advice: Please contact reception on 01225 613100 for a referral
Who to see: GP, Physician Associate/Advanced Nurse Practitioner or Nurse
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: GP or Advanced Nurse Practitioner
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: Advanced Nurse Practitioner, Treatment Room Nurse or Community Pharmacy Referral (minor burns)
Advice: Please contact reception on 01225 613100 to make an appointment/referral
Who to see: GP
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: Treatment Room Nurse
Advice: Once you have received your invitation by post from the NHS, please make an appointment with the Nurse
Who to see: GP or Advanced Nurse Practitioner
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: Nurse
Advice:Baby Clinic is run by our Practice Nurses, appointments needed for Immunisations. Find our more at: www.nhs.uk
Who to see: GP or Nurse (for recall appointments)
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: Research Nurse or Study Co-Ordinator
Advice: Please contact the Research Team on 01225 423250 or email trials.oldfield@nhs.net
Who to see: Community Pharmacy Referral, visit to your local Pharmacy or Self Help - NHS Choices website
Find out more at: www.nhs.uk
Advice: Please contact reception on 01225 613100 to make an appointment/referral
Who to see: Community Pharmacy Referral, visit to your local Pharmacy or Self Help - NHS Choices website
Find out more at: www.nhs.uk
Advice: Please contact reception on 01225 613100 to make an appointment/referral
Advice: Antibiotics are not needed for the common cold as colds are caused by a virus.
Who to see: Community Pharmacy Referral in first instance, if symptoms continue, speak to a GP
Advice: Please contact reception on 01225 613100 to make an appointment/referral
Who to see: Family Planning Clinic or Nurse
Advice: Contraception and family planning appointments are available at various times every day.
Who to see: Community Pharmacy Referral, visit to your local Pharmacy or Self Help - NHS Choices website
Find out more at: www.nhs.uk
Advice: Please contact reception on 01225 613100 to make an appointment/referral
Advice: Antibiotics are not needed for a cough are caused by a virus.
If symptoms persist for more that 3 weeks, please contact the Surgery for a GP appointment
Who to see: Community Pharmacy Referral, visit to your local Pharmacy or Self Help - NHS Choices website
Find out more at: www.nhs.uk
Advice: Please contact reception on 01225 613100 to make an appointment/referral
If symptoms persist, please contact the Surgery for a GP appointment
Who to see: Dentist
Advice: Please book an appointment with your dentist, or find a Dentist service near you: www.nhs.uk
Who to see: GP or Advanced Nurse Practitioner
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: Nurse or GP
Advice: Routine annual clinic appointments will be sent to all our patients with diabetes the month of their birthday. Patients are encouraged to book an appointment with our diabetes specialist nurse or their GP if they have any concerns at any other time and not to wait for their annual review. www.bathdiabetes.org
Who to see: Community Pharmacy Referral, visit to your local Pharmacy or Self Help - NHS Choices website
Find out more at: www.nhs.uk
Advice: Please contact reception on 01225 613100 to make an appointment/referral
If symptoms persist, please contact the Surgery for a GP appointment
Please do not attend the Surgery with Diarrhoea.
Who to see: Nurse / Health Care Assistant
Advice: Please make an appointment with a nurse or healthcare assistant to discuss e.g. weight, exercise, diet, smoking etc.
Who to see: GP or Advanced Nurse Practitioner
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: Nurse
Advice: You may not need to see a clinician in the first instance - find out more at www.nhs.uk. If you think you may need ear irrigation ('syringing')please speak to one of our nurses who will advise you.
Who to see: Community Pharmacy Referral, visit to your local Pharmacy or Self Help - NHS Choices website or our Advanced Nurse Practitioner
Find out more at: www.nhs.uk
Advice: Please contact reception on 01225 613100 to make an appointment/referral
Who to see: Advanced Nurse Practitioner, Community Pharmacy Referral or GP
Advice: Please contact reception on 01225 613100 to make an appointment/referral
Who to see: Community Pharmacy Referral or visit to your local Pharmacy (you can buy over the counter)
Advice: Please contact reception on 01225 613100 to make an appointment/referral
Who to see: Community Pharmacy Referral, visit to your local Pharmacy or Self Help - NHS Choices website
Find out more at: www.nhs.uk
Advice: Please contact reception on 01225 613100 to make an appointment/referral
If symptoms persist, please contact the Surgery for a GP appointment
Who to see: Advanced Nurse Practitioner or GP
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: A new sick note has to be requested via a GP telephone appointment, if it is a repeat sick note, please ask the Receptionist
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: speak to a GP
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: Inform the Receptionist
Advice: Completion of forms, certificates and medicals are not covered under the NHS. You will be charged for these services. Please discuss your requirements with our reception team. Examples are insurance reports, HGV medicals, holiday cancellation forms.
Who to see: Nurse or GP
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: Nurse or GP
Advice: For general advice please ring to book a Telephone Consultation, you will be asked to give the phone number you want to be contacted on and given an approximate time to expect the call, please be available at that time and if using a mobile please ensure it is switched on.
Who to see: Nurse or GP
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: Pharmacist
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: Nurse
Advice: Please contact reception on 01225 613100 to make an appointment
Oldfield Surgery
Who to see: Pharmacist or Nurse
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: Inform the Receptionist
Advice: Holiday Cancellation forms are not covered by the NHS, there will be a charge for this service. Please read the form carefully and fill in and sign any parts that you need to complete before you bring the form to the surgery. We ask that you allow up to 21 days for the process to be completed, you will be contacted by phone when your form is ready for collection.
Who to see: GP
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: Pharmacists
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: Nurse
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: Nurse
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: Pharmacists
Who to see: Pharmacists
Who to see: Inform the Receptionist
Advice: Completion of forms, certificates and medicals are not covered under the NHS. Please read the form carefully and fill in and sign any parts that you need to complete before you bring the form to the surgery. We ask that you allow up to 21 days for the process to be completed, you will be contacted by phone when your form is ready for collection.
Who to see: Inform the Receptionist
Advice: Completion of forms, certificates and medicals are not covered under the NHS. Please read the form carefully and fill in and sign any parts that you need to complete before you bring the form to the surgery. We ask that you allow up to 21 days for the process to be completed, you will be contacted by phone when your form is ready for collection.
Who to see: Nurse or GP
Advice: Please contact reception on 01225 613100 to make an appointment
Oldfield Surgery
Who to see: GP
Advice: Please contact reception on 01225 613100 to make an appointment
St James's Surgery
Who to see: Nurse
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: Nurse or GP
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: Nurse of Health Visitor
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: Nurse or GP
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: Nurse
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: Nurse or GP
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: Nurse or GP
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: GP
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: Nurse or GP
Advice: Please contact reception on 01225 613100 to make an appointment
Oldfield Surgery
Who to see: Nurse or GP
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: Nurse / Health Care Assistant
Advice: Make an appointment with one of our Nurses or health care assistants.
Who to see: Nurse or GP
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: Inform the Receptionist
Advice: Telephone to speak to our reception team. You will be required to give them your exact requirements.
Who to see: Inform the Receptionist
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: Nurse or GP
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: Nurse or GP
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: Please ask reception
Advice: Please ask our reception team who will send your details to our Health Care Assistant who will contact you. If you would like help sooner please visit www.nhs.uk/smokefree and Quit Now!
Who to see: Community Pharmacy Referral, Nurse or GP
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: Nurse or GP
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: Pharmacist, Nurse or GP
Advice: Please contact reception on 01225 613100 to make an appointment for Nurse of GP
Who to see: Pharmacists
Who to see: Self Treatment/Pharmacist
Advice: If worsening please contact the Surgery reception on 01225 613100 to make an appointment to get advice from a clinician.
Who to see: Nurse or GP
Advice: Please contact reception on 01225 613100 to make an appointment
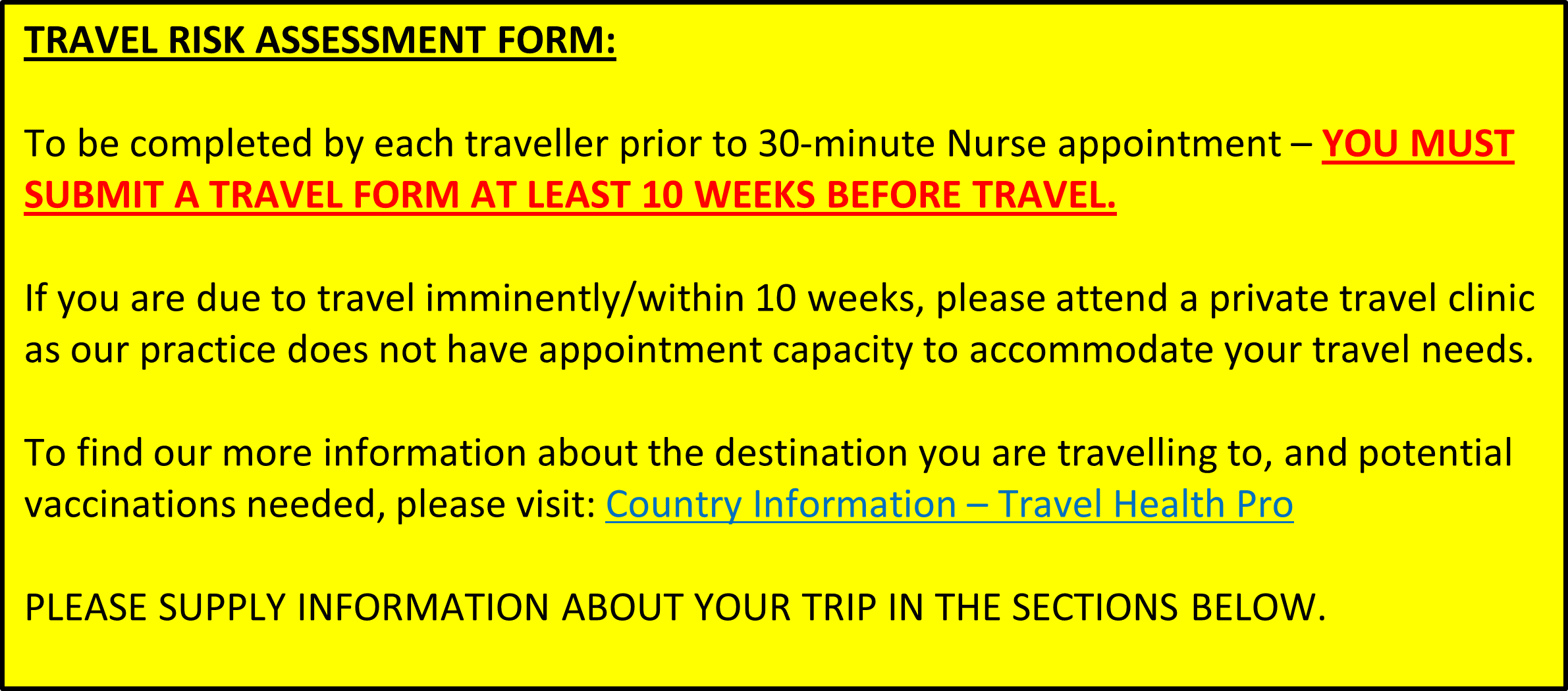
Who to see: Nurse
Advice: Make an appointment to discuss all your travel health needs.
Who to see: Community Pharmacy Referral or visit to a local Pharmacy (Boots Southgate or Preddy Newco Moorland Rd only) if eligible. Must be female, aged between 16-64years old and have 2 or 3 of the following symptoms: Dysuria (painful/difficult urination), New nocturia (urination at night), Urine cloudy to the naked eye. If not eligible as above, or if pregnant, breastfeeding or have visible blood in the urine, then please see a Nurse or GP.
Advice: Please contact reception on 01225 613100 to make an appointment
Oldfield Surgery
Who to see: Nurse
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: Pharmacist
Who to see: Nurse or GP
Advice: Please contact reception on 01225 613100 to make an appointment
Who to see: Pharmacist
Find out more about
symptoms and conditions.
Find out about other services and useful links.